

Abstract
Introduction: COMPLEMENT 2 is a phase III, randomized, open-label study, which compared the efficacy of ofatumumab (OFA) in combination with fludarabine and cyclophosphamide (FC) vs FC therapy alone in patients (pts) with relapsed chronic lymphocytic leukemia (CLL). In a previous interim analysis (2015) performed based on 194 progression-free survival (PFS) events, OFA+FC showed significant improvement of PFS and was well tolerated compared to FC in pts with relapsed CLL. Here, we report the 5-year follow-up of overall survival (OS) and safety profile of the drugs evaluated in this study.
Methods: Based on stratification factors (number of prior CLL therapies and Binet stage), pts with relapsed CLL were randomized 1:1 to Arm A (OFA+FC) and Arm B (FC alone). Arm A received OFA intravenously (IV) (300 mg on day 1, cycle [c] 1; 1000 mg on day 8, c1; and 1000 mg on day 1, c2-6) in addition to FC (F [IV]: 25 mg/m2 and C [IV]: 250 mg/m2 on days 1-3, c1-6). Arm B received FC only. Pts who had achieved a complete response or partial response following at least 1 prior CLL therapy, but whose disease had progressed after >6 months (mo) were included in the present study. The primary endpoint was PFS. Key secondary endpoints were OS, time to next treatment (TTNT), and safety. During the primary analysis for PFS, all the type 1 error (1-sided alpha 0.025) was spent, resulting in no alpha remaining for inferential interpretation of the final analysis for OS. The final analysis results will be used for descriptive and supportive purposes only.
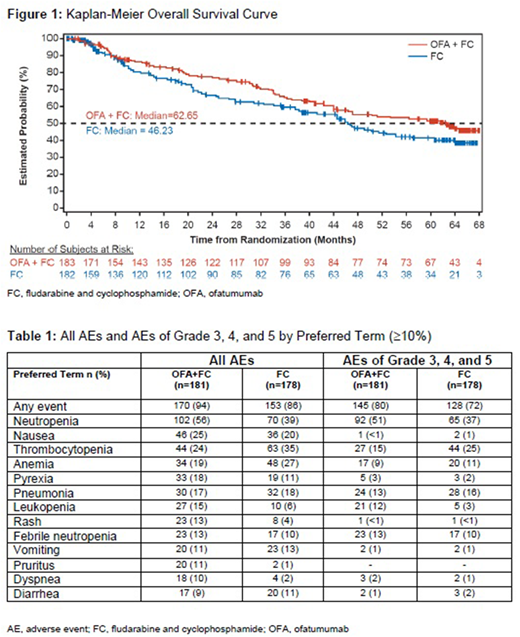
Results: A total of 365 pts were randomly assigned to receive OFA+FC (n=183) or FC (n=182) in the final analysis. Overall, 119 (65%) and 102 (56%) pts completed the scheduled OFA+FC and FC treatments, respectively. Adverse events (AEs) were the main reason for treatment discontinuation in both treatment arms (50 [27%] pts in the OFA+FC arm and 52 [29%] in the FC arm). A total of 332 (91%) pts entered the follow-up phase, 172 (94%) from the OFA+FC arm and 160 (88%) from the FC arm. The follow-up phase for the OFA+FC and FC arms was approximately 41 mo and 23 mo, respectively. Baseline characteristics were similar in both arms. Median PFS was not assessed for the final analysis because the final results for the primary endpoint of PFS were reported as part of the primary analysis. PFS was 28.9 mo for OFA+FC and 18.8 mo for FC (hazard ratio [HR]=0.67, 95% confidence interval [CI]: 0.51, 0.88; p=0.0032). The final OS analysis was performed based on 82 events in the OFA+FC arm and 83 events in the FC arm. Median OS was 62.6 mo (95% CI: 44.58, NA) and 46.2 mo (95% CI: 37.72, 56.57) for the OFA+FC and FC arms, respectively (HR=0.80, 95% CI: 0.59, 1.09; p=0.143) (Figure 1). Median TTNT in the OFA+FC and FC arms was 53 mo and 40.1 mo, respectively (HR=0.77, 95% CI: 0.55, 1.08; p=0.114). As per the primary analysis, the overall response rate (95% CI) by independent review committee assessment (IRC) was 84% (77%, 89%) for OFA+FC and 68% (60%, 74%) for FC (p=0.0003). Other secondary endpoints (in mo) for OFA+FC vs FC were IRC-assessed median time to response (1 vs 1; HR=1.08, 95% CI: 0.85, 1.37; p=0.45), median duration of response (29.6 vs 24.9; HR=0.77, 95% CI: 0.56, 1.05; p=0.09), and median time to progression (42.1 vs 26.8; HR=0.63, 95% CI: 0.45, 0.87; p=0.004).
All AEs and AEs of grade 3, 4, and 5 by preferred term (≥10%) are presented in Table 1. Serious drug-related AEs (≥2%) in the OFA+FC arm were pneumonia (8%), neutropenia and febrile neutropenia (7% each), and thrombocytopenia, pancytopenia, and pyrexia (2% each). Myelodysplastic syndrome was the most frequently reported secondary malignancy observed in ≥1% of pts (OFA+FC, 3 [2%]; FC, 2 [1%]). A total of 82 (45%) and 83 (47%) pts died during the study in the OFA+FC and FC arms, respectively; 2 (1%) and 6 (3%) died up to 60 days after the end of treatment, and 74 (41%) and 69 (39%) after >60 days. Three (2%) on-treatment deaths were reported in the OFA+FC arm and 4 (2%) in the FC arm.
Conclusion: This final analysis confirmed the results of the primary analysis that addition of OFA to FC resulted in improvement of OS and TTNT by approximately 16 mo and 13 mo, respectively, compared to FC alone. Of note, the trend in the OS improvement seems to be maintained in the present long-term follow-up at 5 years. No new safety concerns have emerged in the long-term follow-up after treatment with OFA+FC, and the treatment was well tolerated.
Grosicki:Affimed: Research Funding. Lech-Maranda:Roche: Consultancy; Jansen-Cilag: Consultancy; Novartis: Consultancy; BMS: Consultancy; Amgen: Consultancy. Loscertales:Janssen: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria. Homenda:Janssen: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Rigel: Consultancy, Honoraria; Roche: Consultancy, Honoraria; Acerta: Consultancy, Honoraria. Blonski:Novartis: Consultancy. Stefanelli:Novartis: Employment, Equity Ownership. Vincent:Novartis: Employment. Banerjee:Novartis: Employment. Robak:AbbVie, Inc: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Gilead: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal